delta dental application form
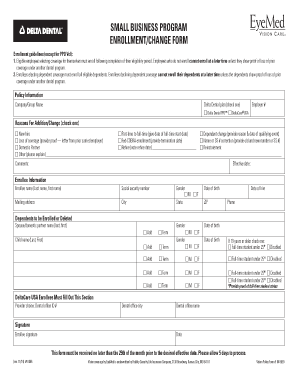
If your company does not currently have a DeltaVision Plan and you would like to learn more about it please contact your producer or Northeast Delta Dental at 1-800260-3788 in Maine 1. Use this form to update the status of your practice as a DeltaCare provider.
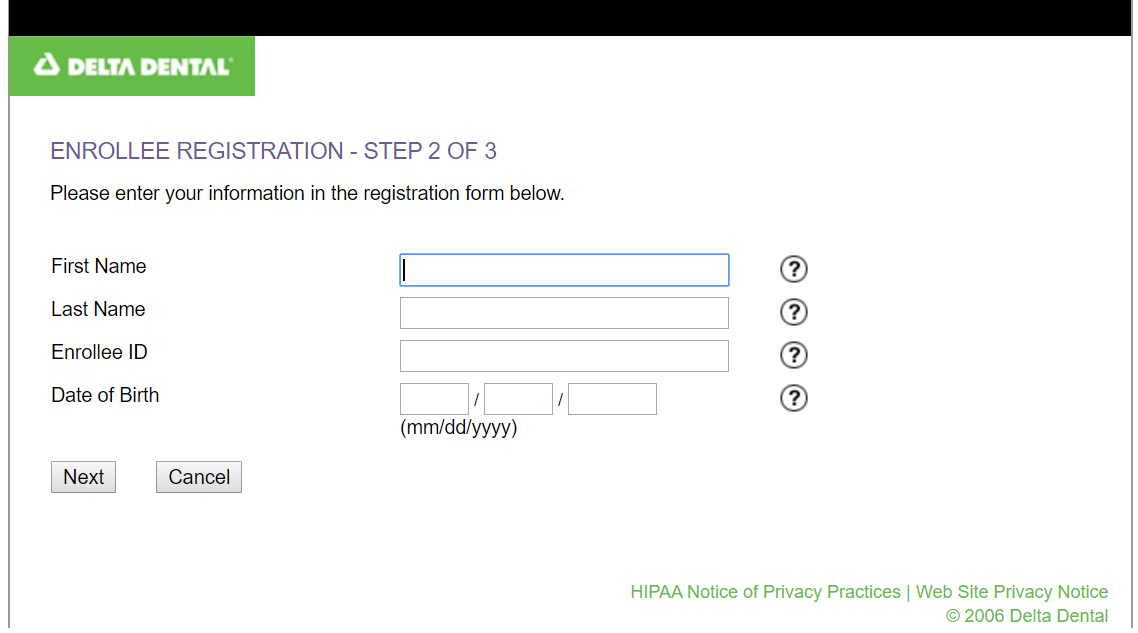
Delta Dental Enrollment Fill Online Printable Fillable Blank Pdffiller
Removable prosthodontics assessment form.
. This form is not needed for. Join our dentist network. Delta Dental is Americas largest and most trusted dental benefits carrier.
We cover more Americans than any other dental benefits provider - and strive to make dental coverage more. Direct Debit Authorization ACH Form. Sale of practice notification form.
DeltaVision HIPAA Form 14b ASO Groups. Standard ADA dental claim forms will also be accepted by the Administrator. More Americans choose Delta Dental than any other dental insurance provider.
Authorization Agreement for Automatic Payments. Continuous orthodontic coverage form for DeltaCare USA. Easily download and submit the form or application that relates to your needs.
Dental Plan Features Add Ons. Box 981400 Boston Massachusetts 02298-1400 Please print or type. They can also call Customer Service at 877 395-9420 or send an email to.
Dentist directory update form. Prepare for Your Dental Appointment. When your tooth or jaw pain just cant wait our care teams are standing by to help.
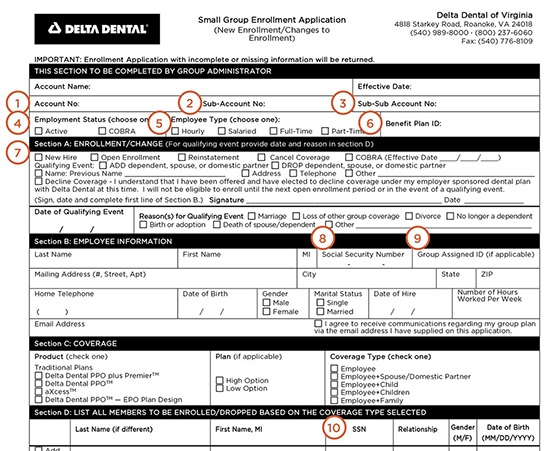
Required fields are starred and must be. Small group employee enrollment form. To access a dental claim form enrollees can log into Member Portal.
MNND Eligibility EnrollmentUpdate Form. DeltaCare Specialty Referral Form Use this form to refer your patient to a specialist. Thats why most dentists choose to work with Delta Dental to protect their patients.
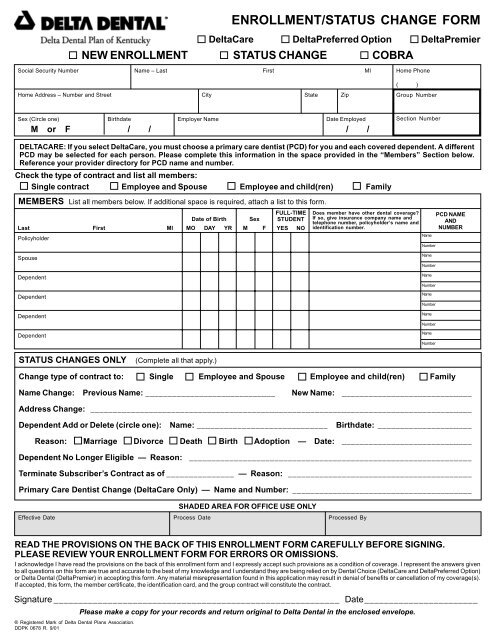
For your own information and protection certain facts should be pointed out to you which could affect your. Use a separate form for each. MN Membership Enrollment Form Spanish Small Group Pooled MN ND Enrollment Form for.
Application and Change Form for Individual Family Dental Insurance PO. DeltaVision HIPAA Form 14a Risk Groups. Call 866 494-4988 or walk into your nearest Aspen Dental office and we will do.
Complete the employees portion of the claim form for dental expense benefits. Issued by Delta Dental you must sign and return this form with your application.
Delta Dental Of Washington Dental Insurance Delta Dental Of Washington
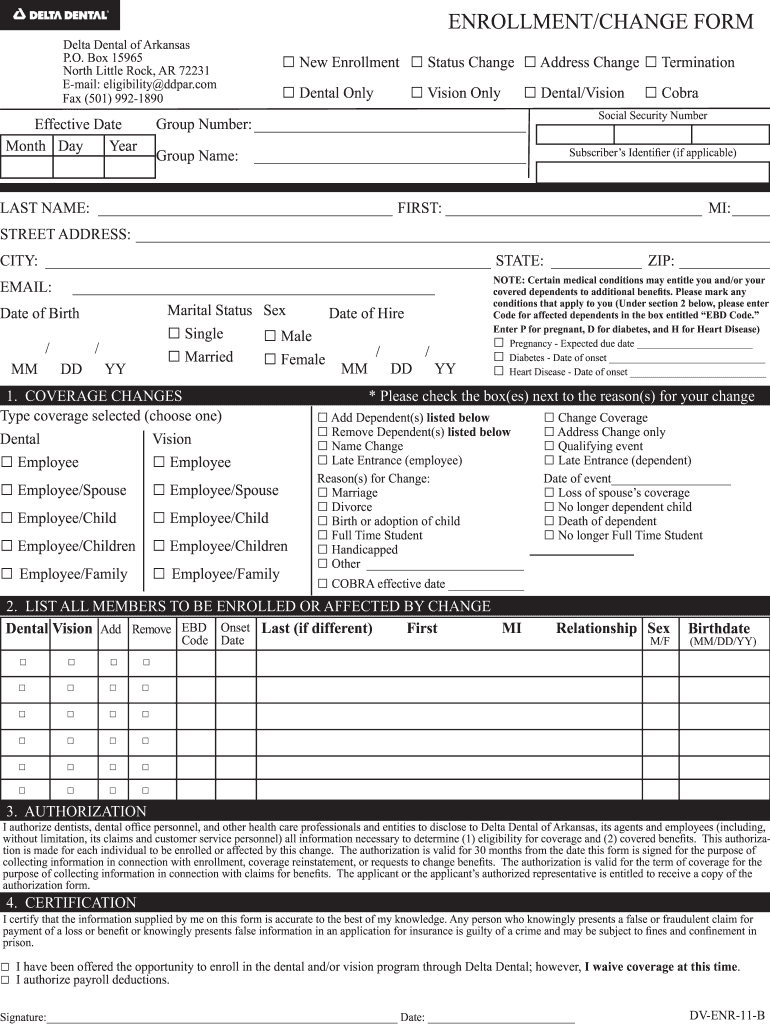
Delta Dental Of Arkansas Enrollment Forms Fill Out Sign Online Dochub
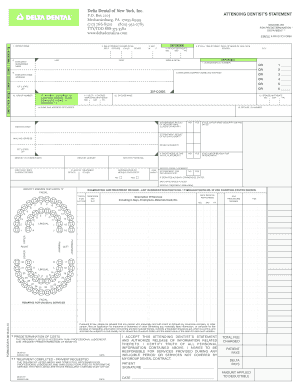
Delta Dental Printable Claim Form Fill Online Printable Fillable Blank Pdffiller
Delta Dental Claim Form Fill Out And Sign Printable Pdf Template Signnow
Dental Insurance

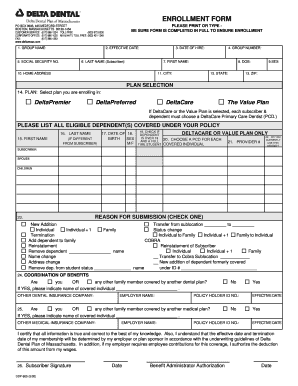
Delta Dental Enrollment Form
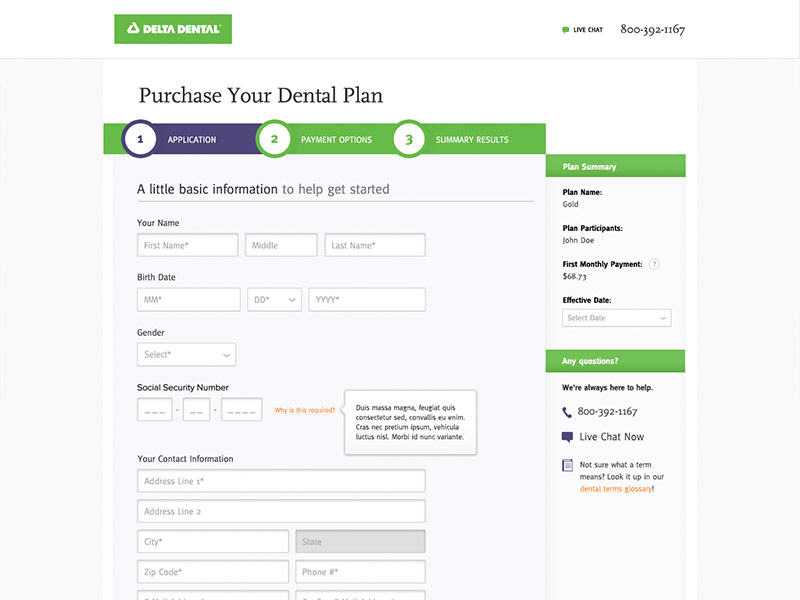
Delta Dental Missouri Application Form By Suejanna On Dribbble

Dental Insurance Forms Delta Dental Of Washington

Delta Dental Claim Form Fill Out And Sign Printable Pdf Template Signnow

Delta Dental New Patients Rubal Dentistry

Delta Dental 101
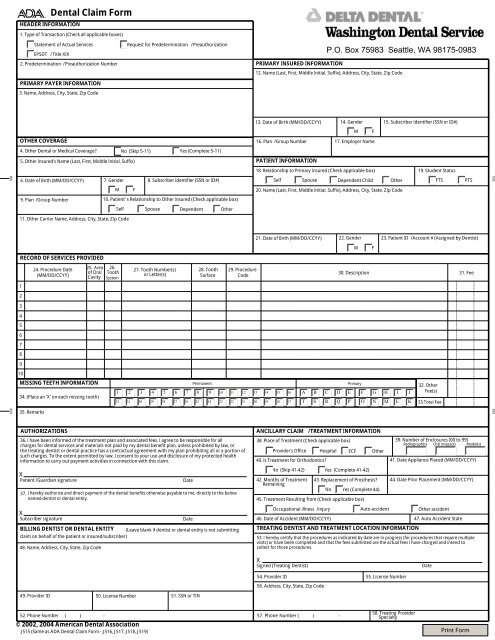
Delta Dental Claim Form Washington Dental Service
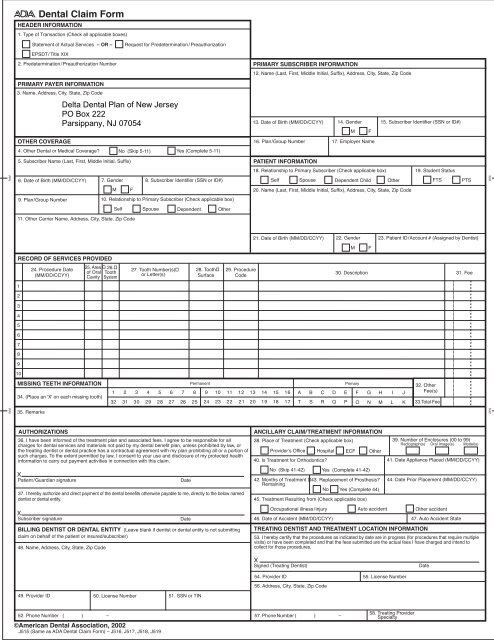
Delta Dental Claim Form
Enrollment

Delta Dental Dental Insurance Dr Robert A Whitmore
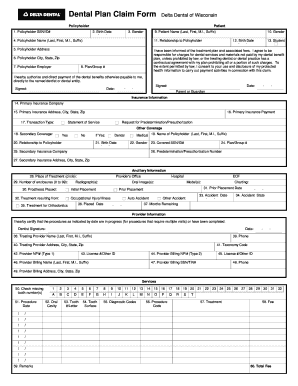
Fillable Online Dental Claim Form Delta Dental Of Wisconsin Fax Email Print Pdffiller
Delta Dental Enrollment Form
Dental Insurance

Claim And Administrative Forms Delta Dental